Sympathetic vs. Parasympathetic: Why “Stress” is the Wrong Explanation

Most people are told the same thing when they feel unwell but tests come back normal:
“You’re probably just stressed.”
While stress can absolutely affect health, this explanation is often incomplete and misleading. It collapses a complex physiological control system into a vague psychological label, and in doing so, it obscures what is actually happening inside the body.
To understand why, we need to look more closely at how the autonomic nervous system really works.
Two systems, one goal: regulation
The autonomic nervous system is made up of two primary branches that are active at all times.
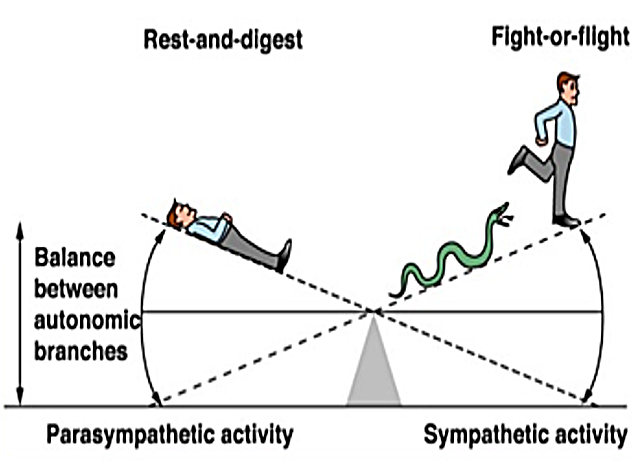
The sympathetic nervous system prepares the body for action. It increases heart rate, raises blood pressure, mobilizes energy, and sharpens attention. This system is essential for waking up, standing upright, exercising, and responding to challenges.
The parasympathetic nervous system restores the body. It slows the heart, supports digestion, regulates hormones, dampens inflammation, and enables recovery after stress. It is the system that allows sleep, healing, and long-term resilience.
Health does not depend on one system being “on” and the other being “off.” It depends on how precisely they coordinate.
This ability to shift, recover, and adapt is called autonomic flexibility.
When the seesaw breaks
Autonomic regulation is often described as a seesaw: when one branch rises, the other falls. In reality, dysfunction is rarely that clean.
In many conditions, the two branches become uncoupled.
One common pattern is what clinicians describe as a “broken seesaw.” Instead of parasympathetic activity withdrawing during stress, it abnormally spikes. This creates excessive braking at the exact moment the body needs to mobilize. To compensate, the sympathetic system is forced to over-fire just to maintain basic function.
The result is a paradoxical state where both systems are highly active at the same time.
People in this state often feel exhausted yet overstimulated, calm yet unable to rest, or “burned out” despite minimal activity. This is not psychological stress. It is a regulatory mismatch.
Not all dysfunction is “high stress”
Another common failure pattern is sympathetic withdrawal, which looks nothing like being anxious or wired.
In this state, the sympathetic system fails to constrict blood vessels appropriately when a person stands. Blood pools in the legs, cerebral blood flow drops, and the brain briefly lacks oxygen, even though the heart may be beating normally or rapidly.
To prevent fainting, the body triggers emergency adrenaline surges.
These surges produce palpitations, tremors, and a sense of dread that are often labeled as panic or anxiety. But there may be no emotional trigger at all. The sensation is physiological, not psychological.
The nervous system is firing adrenaline to preserve consciousness.
The “tired but wired” paradox
Many people describe a particularly confusing symptom pattern: deep fatigue paired with sleeplessness or inner tension.
This often reflects parasympathetic excess coexisting with sympathetic excess.
Parasympathetic overactivity can drive fatigue, low motivation, and depression-like symptoms. At the same time, compensatory sympathetic activation prevents true rest, blocking the natural evening shift required for sleep.
The body feels exhausted, but the nervous system never fully downshifts.
This is why rest alone often fails to restore energy.
Why “stress” hides what matters
The word “stress” hides critical distinctions.
It blurs the difference between:
Autonomic tone (baseline state)
Responsiveness (reaction to challenge)
Recovery (speed of return to baseline)
Flexibility (ability to adapt repeatedly)
Someone may appear calm at rest yet have a brittle nervous system that collapses under mild challenges like standing, deep breathing, or cognitive effort. Standard tests taken at rest often miss this entirely.
What matters is not how stressed someone feels, but how their nervous system behaves over time.
The illusion of heart rate variability
Heart rate variability (HRV) is often used as a proxy for nervous system health. While useful, it has limits.
HRV is a mixed signal. It combines sympathetic and parasympathetic activity into a single number. Two people can have identical HRV scores while having very different autonomic patterns.
For example, a low breathing rate can artificially inflate HRV, masking dangerous sympathetic dominance. Without separating branch-specific activity and analyzing respiratory coupling, critical information is lost.
This is why measuring regulation requires more than a single metric.
From stress management to system assessment
If symptoms were purely psychological, relaxation techniques alone would be sufficient.
But when regulation itself is impaired, the solution begins with understanding:
Which branch is overactive or suppressed
Whether compensatory patterns are driving symptoms
How quickly the system recovers after challenge
Whether flexibility is intact or lost
These questions cannot be answered by symptom checklists or static tests. They must be measured.
At Autonomic Health, the focus is on making this level of physiological insight accessible, so individuals and clinicians can move beyond vague stress narratives toward concrete understanding.
Why this matters for long-term health
Chronic autonomic imbalance does not stay confined to symptoms.
Over time, impaired regulation is associated with inflammation, metabolic dysfunction, cardiovascular strain, immune dysregulation, and reduced resilience to illness. By the time traditional tests show abnormalities, the nervous system has often been compensating for years.
Identifying imbalance earlier opens the door to prevention rather than damage control.
Rethinking stress
Stress is not the enemy. A nervous system that cannot regulate stress is.
Understanding the difference explains why so many people feel unwell without obvious disease and why one-size-fits-all advice often fails.
The future of care lies in measuring regulation, not just managing symptoms.
Autonomic testing is coming soon
At-home autonomic testing is currently in development.
You can sign up on our website to be notified when testing becomes available and learn how your sympathetic and parasympathetic systems are actually functioning.
Because the most important question is not how stressed you feel, but how well your nervous system adapts.
Selected references (for those who want to go deeper)
Goldberger JJ, Arora R, Buckley U, Shivkumar K. Autonomic Nervous System Dysfunction: JACC Focus Seminar.Journal of the American College of Cardiology (2019).
Colombo J, Arora RR, DePace NL, Vinik AI. Clinical Autonomic Dysfunction: Measurement, Indications, Therapies, and Outcomes. Springer (2014).
DePace NL, Colombo J. Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body Wellness. Springer (2019).
Vinik AI, Erbas T, Casellini CM. Diabetic autonomic neuropathy and the autonomic nervous system. Journal of Diabetes Investigation (2013).
Freeman R. Assessment of cardiovascular autonomic function. Clinical Neurophysiology (2006).
Aysin B, Aysin E, Colombo J. Separation of sympathetic and parasympathetic components of heart rate variability using advanced signal processing. IEEE Engineering in Medicine and Biology Conference (2007).
Curtis BM, O’Keefe JH. Autonomic tone as a cardiovascular risk factor. Mayo Clinic Proceedings (2002).